

















The ALS world was invigorated with the FDA approval of Amylyx’ (AMLX) Relyvrio on September 29th. The action brings the number of available ALS medicines to three, adding to riluzole and edaravone. While each of the products only provides a limited benefit, each also represents an advance in treatment and provides a foundation for future breakthroughs. As a follow on to the first chapter in our series and to help readers and stakeholders better understand the disease, we describe ALS, its diagnosis, types and genetic underpinnings in Part II of The ALS Curveball.
What is ALS?
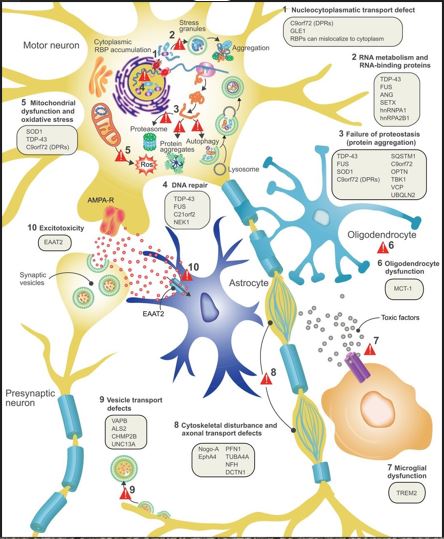
Amyotrophic Lateral Sclerosis is a degenerative neuromuscular disease that affects nerve cells in the central nervous system. It is characterized by progressive degeneration of motor nerve cells in the brain (upper motor neurons) and spinal cord (lower motor neurons). The disease causes physical disability and can produce cognitive decline in almost half of patients. The decline is likely attributable to the development of an ALS form of tau pathology.[1],[2] In a majority, it presents a limited impact on an individual’s intellectual reasoning, vision, hearing, or sense of taste, smell and touch. ALS is a primary central and peripheral nervous system degenerative disorder with a secondary inflammatory component.

ALS has two primary types of onset: limb and bulbar. Limb onset presents itself with a combination of upper and lower motor neuron signs in the limbs while bulbar is characterized by speech and swallowing difficulties, with limb features developing later in the disease. Symptoms of the disease include twitching and cramping of muscles, especially those in the hands and feet, fasciculations in multiple muscle groups, loss of motor control in the hands and arms, impaired use of the arms and legs, weakness and fatigue, tripping and falling among others related to the weakness and uncertainty of muscle use. As the disease progresses, patients may suffer shortness of breath, difficulty breathing and swallowing and paralysis.
A patient afflicted with ALS usually dies due to loss of respiratory function. Lack of nutrition had historically been another cause of death; however, standard of care now employs nasogastric feeding tubes and parenteral nutrition. Survival is brief and 50% die within 30 months of symptom onset and only 10% survive more than ten years. In general, the later the onset of ALS, the shorter the survival.
The disease occurs throughout the world in all races and ethnicities and is more common in older persons. Environmental, genetic and lifestyle factors are all thought to play a role, although the magnitude of their contribution is unknown. Military service, traumatic head injuries, competitive sports, smoking, toxins and viral infections have all been associated with ALS to some degree, however, the links are tenuous. Biological factors have also been observed to have a correlation with ALS. Higher levels of chemical messenger glutamate, increased inflammation in the brain and misfolded proteins are also implicated in the disease.
Genetic factors are most relevant in Familial ALS, with up to 40% of Familial cases attributable to the C9orf72 gene. Other key genes include TARDBP, FUS and SOD1, which are important for the normal functioning of motor neurons.
Diagnosis
ALS symptoms usually include muscular weakness, slurred speech, or the loss of ability to use fine motor skills. A primary care physician is usually the first health care professional to narrow the likelihood to ALS, followed by a referral to a neurologist.
A neurological exam is conducted which evaluates the extent of muscle weakness, lower and upper neuron function and emotional changes. Diagnostic tests come next and include magnetic resonance imaging (MRI), electromyography (EMG), spinal tap and blood tests.
Disease Types
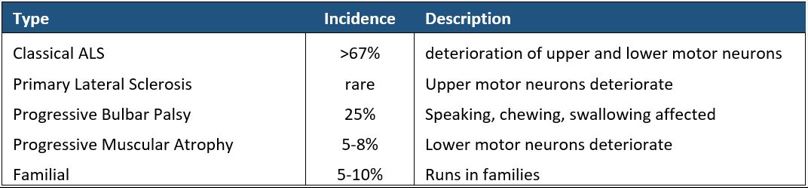
Dr. Charcot, who we introduce in Chapter 1, differentiated among the different stages of ALS, identifying the beginning of the disease in the upper limbs and trunk, followed by the next stage of lower limb rigidity, without bladder involvement. The final stage of the disease is characterized by worsening bulbar symptoms with death occurring two or three years later.[4] Dr. Charcot also separated ALS into other divisions distinguishing classic ALS from progressive muscular atrophy and bulbar paralysis.[5] His other achievements were to be the first to correctly label ALS as a neuropathy rather than a myopathy and the distinction of having his original clinical and anatomical descriptions of ALS persist with little change over the last century and a half. Below we list five categories of ALS and their approximate incidence.

How Common is ALS?
As diseases go, ALS occurs infrequently. Our review observed estimates of incidence ranging from 1 to 5.2 persons per 100,000 depending on study and geography.[6],[7],[8] Prevalence is estimated from 5.2 to 6.0 per 100,000 given the relatively short three-to-five-year lifespan of those diagnosed.[9],[10] In the United States this equates to 5,000 to 6,000 cases per year and about 120,000 around the world.
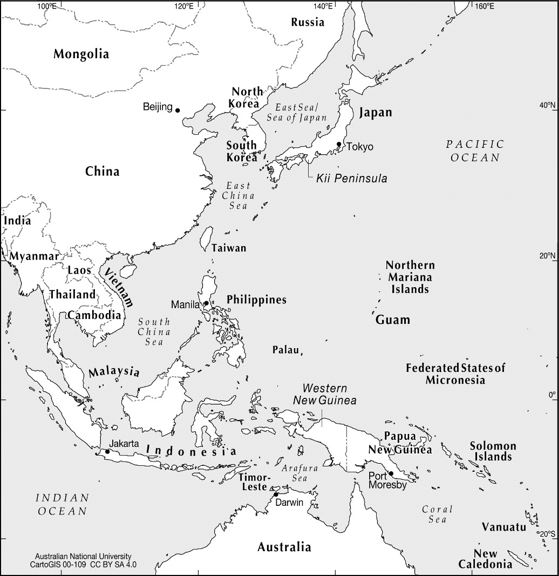
ALS occurs less often in individuals under 40 and more often in those over 70 with an average age of onset between 55 and 60.[11],[12] Men are 20% more likely to suffer from the disease compared to women; however, this discrepancy narrows with age.[13] Caucasians suffer from the disease more frequently than other racial groups and the incidence of the disease had been elevated in Guam, Western New Guinea and parts of the Kii peninsula of Japan.[14] Incidence in these areas has shifted to world averages after the adoption of a Western diet.
![ALS Hotspots: Guam, New Guinea and Japan in Western Pacific [15]](https://i.ibb.co/1fqKsYM/The-ALS-Curveball-2.jpg)
Associated Genes
In 1993, Daniel Rosen of the Massachusetts General Hospital and colleagues identified the first gene mutations related to ALS. Mutations in the gene superoxide dismutase 1 gene (SOD1) were correlated with the pathogenesis of familial ALS. This finding led to the engineering of the first transgenic model of SOD1-G93A mice in 1994 opening up new approaches to research. As of 2021, there are more than 50 genes[16] implicated in the disease and more than 120 genetic variants linked with it.[17] Approximately 90% of ALS cases are sporadic and cannot be directly traced back to ancestry; however, there are numerous genes in combination that are associated with the disease and work is ongoing to identify a genetic fingerprint.
SOD1 mutations lead to the production of intraneural protein aggregates and cause cellular stress and disrupt protein balance. In its normal form, SOD1 converts the superoxide anion to less damaging hydrogen peroxide. However, when mutated, it is hypothesized that the neuron loss is caused by the damage to mitochondrial function and axonal transport. Mutated SOD1 is associated with Familial ALS and is present in 12-20% of inherited cases. In sporadic ALS it comprises 1-2% of the cases.[18],[19] SOD1 mutants may easily misfold and can bind to form aggregates. The mutants are selectively toxic and lead to the death of the upper and lower motor neurons.[20]
Another gene that is associated with ALS is Transactive Response DNA Binding Protein (TARDBP) which codes for the TDP-43 protein. Mutations in this gene are present in about 5% of cases of ALS and are usually associated with cytoplasmic aggregates or inclusions. Notably, TDP-43 is also found in cytoplasmic aggregates in the majority of sporadic ALS cases suggesting a prominent role in the pathogenesis of the disease.
Yet another gene associated with ALS is the Fused in Sarcoma (FUS) gene, which produces a DNA/RNA binding protein. Mutations in this gene are associated with ALS and it is the second most common cause of Familial ALS. Characteristics of FUS-related ALS include an earlier age of onset, more frequent bulbar disease and a more rapid disease progression in contrast to SOD1 related disease.[21]
Although mutations in the genes coding for TDP-43 and FUS are present in only a small percentage of all ALS patients, more than 90% of ALS patients have TDP-43 pathology and the majority of ALS patients have FUS pathology at autopsy. These findings underscore the importance of developing therapies that are capable of reducing the toxicity of these proteins whether or not they are found in their mutated forms.[22]
The chromosome 9 open reading frame 72 (C9orf72) gene is implicated in 25 to 40% of Familial or inherited cases. It was discovered in 2011 and the protein coded in the gene is abundant in areas of the cerebral cortex and spinal cord that control movement. The protein plays a role in the regulation of endosomal trafficking and is involved with other proteins that are involved in autophagy and endocytic transport. Expansion in an area of repeats in the gene sequence for the protein is associated with ALS and frontotemporal dementia (FTD).
Future advancements in the identification of genes associated with ALS will provide more detail about its causes and potentially help identify new therapeutic targets that can help treat and cure the disease.
Coda
ALS is a debilitating disease that removes an individual’s ability to walk, speak and in many cases process thought. Albeit at a slow pace, progress is being made with new medicines receiving approval. As our understanding of the causes and genetic components of ALS improve, we expect to see an acceleration in new treatments. In our next chapter, we will further examine available therapies and review the leading candidates in development for ALS, highlighting some of the most promising.
[0] Featured Photo: National Human Genome Research Institute. Coding region in a segment of eukaryotic DNA.
[1] ALS, Cognitive Impairment & Dementia. A Professional’s Guide from the ALS Association. June 2020.
[2] Denis Kay, Ph.D. Department of Pathology and Microbiology at the Atlantic Veterinary College, UPEI.
[3] Philip Van Damme P, Robberecht W, Van Den Bosch L (May 2017). "Modelling amyotrophic lateral sclerosis: progress and possibilities." Disease Models and Mechanisms. 10 (5): 537-549. doi:10.1242/dmm.029058 PMC: 5451175 PMID: 28468939. This file is licensed under the Creative Commons Attribution 3.0 Unported license.
[4] Katz, J. et al. Amyotrophic Lateral Sclerosis: A Historical Perspective. Neurol Clin 33 (2015) 727–734 http://dx.doi.org/10.1016/j.ncl.2015.07.013
[5] Katz, J. et al. Amyotrophic Lateral Sclerosis: A Historical Perspective. Neurol Clin 33 (2015) 727–734 http://dx.doi.org/10.1016/j.ncl.2015.07.013
[6] Talbott, E.O., Malek, A.M., Lacomis, D. The epidemiology of amyotrophic lateral sclerosis. Handbook of Clin Neurology. 2016;138:225-38. doi: 10.1016/B978-0-12-802973-2.00013-6.
[7] Amyotrophic lateral sclerosis. MedlinePlus, National Library of Medicine.
[8] Xu, L. et al. Global variation in prevalence and incidence of amyotrophic lateral sclerosis: a systematic review and meta-analysis. J Neurol. 2020 Apr;267(4):944-953. doi: 10.1007/s00415-019-09652-y.
[9] Talbott, E.O., Malek, A.M., Lacomis, D. The epidemiology of amyotrophic lateral sclerosis. Handb Clin Neurol. 2016;138:225-38. doi: 10.1016/B978-0-12-802973-2.00013-6.
[10] Mehta, P. et al. Prevalence of Amyotrophic Lateral Sclerosis — United States, 2015. Weekly / November 23, 2018 / 67(46);1285–1289
[11] Alstreatment.com, ALS Incidence.
[12] Talbott, E.O., Malek, A.M., Lacomis, D. The epidemiology of amyotrophic lateral sclerosis. Handbook of Clin Neurology. 2016;138:225-38. doi: 10.1016/B978-0-12-802973-2.00013-6.
[13] How Common is ALS? ALS News Today.
[14] Kihira, T. et al. An increase in ALS incidence on the Kii Peninsula, 1960-2009: A possible link to change in drinking water source. Amyotroph Lateral Scler. 2012 Jun; 13(4): 347–350
[15] Western Pacific. CartoGIS Services, College of Asia and the Pacific, The Australian National University. Used with permission.
[16] Chen, L. et al. SOD1 Mutation Spectrum and Natural History of ALS Patients in a 15-Year Cohort in Southeastern China. Frontiers in Genetics. October 14, 2021. doi: 10.3389/fgene.2021.746060
[17] Hulisz, D. Amyotrophic Lateral Sclerosis: Disease State Overview. American Journal of Managed Care. August 2018.
[18] Hulisz, D. Amyotrophic Lateral Sclerosis: Disease State Overview. American Journal of Managed Care. August 2018.
[19] Siddique, T., Ajroud-Driss, S. Familial amyotrophic lateral sclerosis, a historical perspective. Acta Myologica. October 2011.
[20] Huai, J. and Zhang, Z. Structural Properties and Interaction Partners of Familial ALS-Associated SOD1 Mutants. Frontiers in Neurology, May 2019.
[21] Yan, J. et al. Frameshift and novel mutations in FUS in familial amyotrophic lateral sclerosis and ALS/dementia. Neurology. 2010 Aug 31; 75(9): 807–814.
[22] Denis Kay, Ph.D. Department of Pathology and Microbiology at the Atlantic Veterinary College, UPEI.





{kind=link}